

Greater than 67 million individuals—20% of the U.S. population—obtain their medical insurance protection by means of the federal Medicare program. Among the many mostly used companies that Medicare covers are doctor companies and different outpatient companies lined underneath Medicare Half B. In 2021, 9 out of 10 beneficiaries in conventional Medicare used doctor and different Half B medical companies. Nearly half of the $1 trillion in gross Medicare profit spending in 2023 (49% or $493 billion) was spent on Half B companies. Medicare Half B spending accounts for 25% of all national spending for doctor and medical companies.
Annually, the Facilities for Medicare & Medicaid Providers (CMS) updates Medicare funds for doctor companies and different Half B companies by means of rulemaking, primarily based on parameters established underneath legislation. In November 2024, CMS finalized a 2.83% decrease within the physician fee schedule conversion issue, a key facet of doctor fee charges underneath the Medicare program. This resulted in a mean fee minimize of two.93% to physicians and different clinicians, which took impact on January 1, 2025 and stays in impact right now. Congress thought of however didn’t enact laws to reverse the minimize in Medicare doctor funds in the year-end spending bill and within the 2025 continuing resolution that funds the federal government by means of the top of the fiscal yr (Determine 1). Some policymakers proceed to push for a fix, which is reportedly into consideration for inclusion in an upcoming funds reconciliation invoice.
Efforts by lawmakers to handle the Medicare doctor fee minimize for 2025 are the newest in a sequence of legislative actions to supply short-term increases to doctor fee charges underneath Medicare to keep away from comparable reductions in charges. The fee minimize finalized for 2025 follows the expiration of non permanent funds underneath the Consolidated Appropriations Act of 2024, which offered a 2.93% enhance to doctor funds for a portion of 2024 to stave off scheduled cuts.
Through the years, physician groups and some policymakers have known as for broader reforms to stabilize Medicare funds to physicians and different clinicians, and have expressed considerations that instability and lack of income may push physicians to choose out of the Medicare program, creating potential entry issues for Medicare beneficiaries. Physicians should not required to take Medicare sufferers, however most do; virtually all (98%) of non-pediatric physicians settle for Medicare’s commonplace fee fee for all Medicare lined companies, and just 1% opted out of this system in 2024.
MedPAC and others have raised further considerations about points such because the long-standing gap in compensation between major care and specialty care clinicians, the efficacy of quality-based fee incentives by means of the Quality Payment Program (QPP), and the affect of medical specialty teams and pursuits by means of the American Medical Affiliation/Specialty Society Relative Worth Scale (RVS) Replace Committee, in any other case generally known as the RUC. The RUC points annual suggestions to CMS on doctor fee charges, and CMS has traditionally adopted most of those suggestions annually. These points have drawn the attention of policymakers lately, together with Robert Kennedy Jr., the Trump administration’s new Secretary of the Division of Well being and Human Providers (HHS), who has voiced curiosity in facets of Medicare doctor fee reform, resembling growing incentives for major and preventive care, in addition to bringing greater transparency to the operations of the RUC and doubtlessly reducing the AMA’s influence over fee charges.
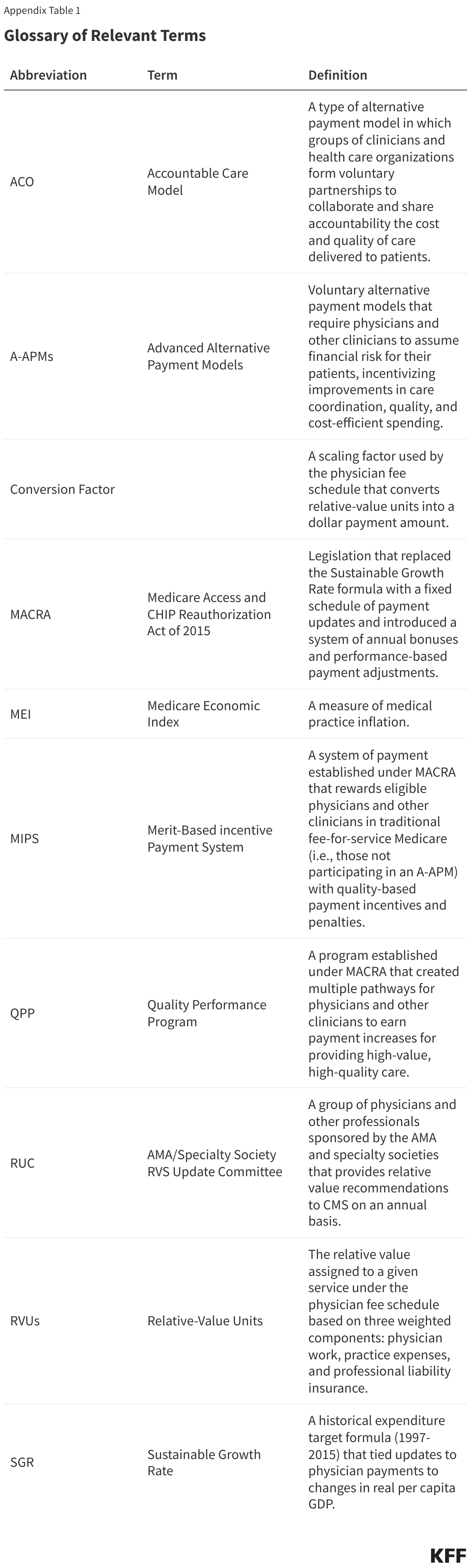
This challenge transient solutions key questions on how Medicare pays physicians and different clinicians, and critiques coverage choices underneath dialogue to reform this fee system. The transient is concentrated totally on the doctor fee system utilized in conventional Medicare. Medicare Benefit plans have flexibility to pay suppliers in another way and presently there isn’t any systematic publicly-available data on how a lot Medicare Benefit plans pay suppliers. (See Appendix for a glossary of related applications, laws, and phrases.)
1. What’s the Medicare doctor payment schedule?
Medicare reimburses physicians and different clinicians primarily based on the physician fee schedule, which assigns fee charges for greater than 10,000 health care services, resembling workplace visits, diagnostic procedures, or surgical procedures. For companies offered to conventional Medicare beneficiaries, Medicare usually pays the supplier 80% of the payment schedule quantity, whereas the beneficiary is answerable for a coinsurance of 20%. Physicians who take part in Medicare agree to simply accept this association as fee in full (generally known as accepting “task”) for all Medicare lined companies. Non-participating physicians obtain 5% decrease Medicare funds, however could settle for “task” on a claim-by-claim foundation and should select to invoice beneficiaries for bigger quantities by charging further coinsurance, as much as 15% greater than the Medicare-approved quantity for the price of a lined service. A third group of physicians choose out of the Medicare program altogether, and as a substitute enter into personal contracts with their Medicare sufferers, should not restricted to charging payment schedule quantities, and don’t obtain any reimbursement from Medicare. Only one p.c of all non-pediatric physicians opted out of the Medicare program in 2024.
Doctor payment schedule charges for a given service are primarily based on a weighted sum of three parts: (1) clinician work, (2) observe bills, and (3) skilled legal responsibility insurance coverage (also called medical malpractice insurance coverage). These three parts are measured when it comes to “relative worth items” (RVUs). Collectively these three parts symbolize the general price and energy related to a given service, with extra pricey or time-intensive companies receiving a better weighted sum. Every part is adjusted to account for geographic variations in enter prices, and the result’s multiplied by the payment schedule conversion factor (an yearly adjusted scaling issue that converts numerical RVUs into fee quantities in {dollars}). Charge schedule companies are every related to a singular service code, which permits clinicians to hunt reimbursement for the care they supply on a service-by-service foundation.
Cost charges specified underneath the doctor payment schedule set up a baseline quantity that Medicare pays for a given service, however funds could also be adjusted primarily based on different components, resembling the positioning of service, the kind of clinician offering the service, and whether or not the service was offered in a chosen health professional shortage area. Physicians can even obtain quality-based fee changes underneath the Quality Payment Program (QPP) (see question 7).
2. How does Medicare replace doctor fee charges?
Annual updates to the doctor payment schedule embody statutorily-required updates to the conversion issue underneath the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) (see question 6), in addition to different changes to replicate the addition of recent companies, modifications in enter prices for current companies, and different components. Included in these changes are periodic modifications to the RVUs assigned to payment schedule service codes, primarily based partly on the suggestions of a multispecialty committee of physicians and different professionals, generally known as the AMA/Specialty Society RVS Update Committee (RUC) (see question 3).
Beneath present legislation, the projected price of all modifications to the doctor payment schedule should be funds impartial. That’s, the modifications could not increase whole Medicare spending by greater than $20 million in a given yr. This requirement was established by the Omnibus Budget Reconciliation Act of 1989 to handle considerations that constraints on doctor charges for particular companies would result in will increase in service quantity and development in Medicare spending for doctor companies over time. The legislation requires CMS to regulate payment schedule spending when projected prices exceed the $20 million threshold, usually by reducing the conversion issue relative to the statutory replace known as for by MACRA.
3. What’s the position of the RUC in figuring out doctor fee charges?
The AMA/Specialty Society RVS Replace Committee (RUC) is a volunteer committee of physicians and different professionals, formed by the American Medical Association (AMA) in 1991 to advise CMS on the relative weighting of service codes underneath the doctor payment schedule, the first mechanism utilized by CMS to set relative funds for doctor and medical companies. The RUC is an impartial physique and its operations should not instantly overseen by Congress or CMS. Additional, as a result of the RUC will not be an official federal advisory committee, it isn’t certain by federal standards round transparency, membership steadiness, and different working necessities utilized to many comparable committees. The RUC includes representatives from the AMA and different skilled organizations, in addition to members appointed by a spread of nationwide medical specialty societies.
Annually, CMS identifies doubtlessly misvalued companies for RUC evaluate primarily based on statutory standards and public nomination. Probably misvalued companies may additionally be recognized by the RUC itself, whereas new or just lately revised service codes are recognized by a separate AMA panel, generally known as the Current Procedural Terminology (CPT) Editorial Panel. The RUC then consults with numerous medical specialty societies, who resolve which companies they want to evaluate and develop suggestions on the clinician work, observe bills, and different components related to fee for every service. A closing record of suggestions for reviewed companies is compiled by the RUC primarily based on a committee vote and referred to CMS.
CMS will not be required to undertake suggestions issued by the RUC, nevertheless it does so in a majority of circumstances. The AMA stories a mean annual acceptance fee of 90% from 1993 to 2025. Through the years, MedPAC and others have raised considerations concerning the affect of the RUC, which is basically composed of specialty physicians with a monetary stake within the suggestions they’re producing, and famous a number of methodological points with the information used to develop RUC suggestions (see question 8). MedPAC has known as for CMS to develop internal processes to validate RUC suggestions by impartial means. Extra just lately, HHS Secretary Kennedy has raised concerns concerning the lack of transparency and relative lack of oversight of RUC operations by CMS, in addition to the affect of the AMA in setting fee charges for physicians, which has introduced renewed attention to the problem (see question 9).
4. How have doctor fee charges modified in 2025?
CMS recently finalized fee modifications for 2025, which embody a 2.83% lower to the doctor payment schedule conversion issue relative to 2024. This lower displays the next changes: (1) the expiration of non permanent funds accredited by Congress underneath the Consolidated Appropriations Act of 2024, which elevated funds by 2.93% for all payment schedule companies furnished between March 9, 2024 and December 31, 2024, (2) a 0% statutory enhance for 2025 underneath the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), and (3) a modest 0.02% funds neutrality adjustment. The mixed affect of those changes is a 2.93% lower in common funds to physicians and different clinicians, which went into impact on January 1, 2025.
As of March 2025, Congress has not handed laws to handle this fee minimize. A provision to cut back (although not absolutely get rid of) the minimize was included in an early version of the year-end Persevering with Decision (CR) filed in December 2024, just like the non permanent fee changes instituted by Congress in prior years, however was faraway from the version signed into law. Congress additionally thought of, however did not include, laws within the subsequent CR enacted in March 2025, however some policymakers proceed to push for a fix, which is reportedly into consideration for inclusion in an upcoming funds reconciliation invoice.
5. How did the 2025 fee rule handle points associated to major care, telehealth, and different well being care priorities?
Current modifications to the doctor payment schedule additionally embody a number of measures designed to enhance well being care entry and enhance help for preventive companies, behavioral well being, and administration of continual illness. These measures are part of an ongoing effort by CMS and the Division of Well being and Human Providers (HHS) to strengthen major and preventive care and handle long-standing concerns concerning the hole in compensation between major and specialty care physicians (see question 8). The final payment rule for 2025 introduces the next key modifications:
- CMS has added new billing codes to the doctor payment schedule supposed to streamline fee for advanced primary care management. This transformation bundles a number of current companies associated to care administration, interprofessional session, and different care parts into single codes, stratified by affected person medical and social complexity, which can be billed on a month-to-month foundation.
- CMS has added new billing codes associated to caregiver coaching for direct care companies and helps, permitting clinicians to invoice for time spent coaching caregivers on particular medical expertise resembling strategies to stop ulcer formation, wound dressing modifications, and an infection management, and has expanded current billing choices for trainings devoted to caregiver conduct administration and modification.
- CMS has finalized a number of provisions geared toward enhancing beneficiary entry to telehealth, resembling broader protection of audio-only companies and elevated flexibility in the usage of telehealth for remedy of opioid use dysfunction (OUD). Security planning interventions and PrEP counseling have been added to the Medicare Telehealth Services list on a everlasting foundation, and caregiver coaching companies have been added on a provisional foundation.
- Absent additional motion from Congress, lots of the different telehealth restrictions that have been in place previous to the COVID-19 pandemic will come again into impact on April 1, 2025. These include restrictions limiting telehealth protection to beneficiaries in rural areas, and requiring beneficiaries to journey to an accredited website, such a clinic or physician’s workplace, when receiving telehealth companies. Nevertheless, CMS has prolonged sure restricted flexibilities underneath its authority by means of December 2025, resembling provisions that enable Rural Health Centers (RHCs) and Federally Qualified Health Centers (FQHCs) to function distant website suppliers for all lined telehealth companies, and permit suppliers to make use of their presently enrolled observe location rather than their house handle when offering telehealth companies from house.
- CMS has additionally added new billing codes for a spread of different major and behavioral well being companies, resembling cardiovascular danger evaluation and care administration, use of digital psychological well being remedy gadgets, and security planning interventions for sufferers vulnerable to suicide or overdose, amongst others.
- CMS has finalized a number of updates to the Quality Payment Program (QPP) to enhance the accuracy of high quality reporting and cut back administrative burden for suppliers taking part within the Merit-based Incentive Payment System (MIPS). (For a extra detailed description of the QPP and MIPS, see question 7).
The brand new guidelines additionally embody updates to the Medicare Shared Savings Program (MSSP), a everlasting accountable care organization (ACO) program in conventional Medicare that provides monetary incentives to suppliers for assembly financial savings targets and high quality objectives, in addition to different modifications associated to fee for preventive vaccine administration, opioid remedy applications, analysis and administration of infectious ailments in hospital inpatient or remark settings, and a wide range of different well being companies.
6. How have Medicare funds to physicians modified for the reason that implementation of MACRA?
Medicare has revised its system of fee for doctor companies quite a few occasions through the years (Determine 1). The present fee system was established underneath the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) and contains two major parts: (1) a schedule for annual, statutorily-defined updates to the conversion issue, a key determinant of fee charges underneath the doctor payment schedule, and (2) a brand new system of bonus funds and quality-based fee changes underneath Quality Payment Program (QPP) (see question 7).
The doctor fee system established by MACRA was supposed to stabilize fluctuations in fee brought on by the prior system underneath the Medicare Sustainable Growth Rate (SGR) formula, which set annual targets for Medicare doctor spending primarily based on development within the gross home product (GDP). Beneath the SGR, if doctor spending exceeded its goal in a given yr, fee charges can be minimize the next yr, whereas spending that was beneath the goal led to elevated charges. As with the present system, charges have been topic to additional adjustment for funds neutrality if the projected price of all payment schedule spending was projected to extend by greater than $20 million for the yr.
The SGR was established by the Balanced Budget Act of 1997 to sluggish the expansion in Medicare spending for doctor companies, however the method garnered criticism, as development in service quantity and rising prices led to a number of years of spending on doctor companies that exceeded the expansion goal, necessitating fee cuts from 2002 onward. Between 2002 and 2015, Congress enacted 17 short-term interventions (so-called “doc-fixes”) to delay the cuts and supply non permanent will increase to doctor funds, however did so with out repealing the SGR, which resulted in amassed deficits over time.
MACRA permanently eliminated the SGR method, stopping a 21.2% minimize in doctor charges slated for 2015 and changing it with 0% statutory will increase to the conversion issue by means of 2025 (later raised to 0.5% from 2016-2019), adopted by modest annual will increase from 2026 onward. These updates are set by MACRA and don’t fluctuate primarily based on underlying financial situations. Nevertheless, subsequent changes to protect funds neutrality and supplemental funds offered by Congress could lead to conversion issue updates which might be increased or decrease than the statutorily-required replace in a given yr.
Though MACRA has stabilized funds underneath the doctor payment schedule to a point relative to the years main as much as its enactment, charges have continued to fluctuate over the past decade. Resulting from strict funds neutrality necessities, CMS has restricted flexibility to regulate fee charges for brand new or undervalued companies with out offsetting the prices elsewhere within the payment schedule. This usually takes the type of funds neutrality changes to the conversion issue, resembling a -10.20% adjustment in 2021 and a -2.18% adjustment in 2024. Since 2021, Congress has offered several short-term increases to payment schedule charges to spice up fee throughout the COVID-19 pandemic and to offset budget-neutrality cuts, elevating considerations that the cycle of “doc-fixes” underneath the SGR method has not been wholly prevented underneath MACRA.
7. How does the High quality Cost Program (QPP) issue into doctor funds?
The Quality Payment Program (QPP), which launched in 2017, was established by the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) to create monetary incentives for well being care suppliers to regulate prices and enhance care high quality. The QPP contains two distinct pathways for participation: (1) incentive funds for individuals in certified advanced alternative payment models (A-APMs) and (2) efficiency primarily based fee changes underneath the Merit-based Incentive Payment System (MIPS).
A-APM Incentive Funds: Physicians and different clinicians who take part in certified A-APMs, resembling choose accountable care organizations (ACOs) and others, are eligible for bonus funds in the event that they meet sure participation thresholds. A-APMs are a kind of value-based care mannequin by which the supplier bears some monetary danger for the prices of care in an outlined setting, resembling remedy of a selected situation or major care companies for a bunch of beneficiaries, usually by sharing in a portion of monetary financial savings and losses relative to a benchmark. Incentive funds to extend participation in A-APMs are a part of a broader goal by CMS to have all conventional Medicare beneficiaries in some kind of accountable care relationship by 2030.
Annually, A-APM clinicians qualify for bonus funds primarily based on their participation throughout the Qualifying APM Participant Performance Period (January 1 – August 31) two years prior. Beneath MACRA, qualifying A-APM clinicians obtained a 5% bonus in fee years 2019 by means of 2024 (efficiency durations 2017 – 2022). Congress subsequently prolonged these bonus funds to incorporate a 3.5% bonus in 2025 and a 1.88% bonus in 2026. A-APM bonus funds are scheduled to be phased out in favor of annual 0.75% will increase to the conversion issue for qualifying A-APM clinicians (relative to smaller 0.25% will increase for all different clinicians). These conversion issue updates will start in 2026, and A-APM bonus funds might be absolutely retired in 2027.
Roughly 386,000 clinicians certified for A-APM bonuses in 2024, primarily based on the 2022 efficiency interval, a virtually fourfold enhance from 99,000 in 2019, the primary yr A-APM bonuses have been out there. On the identical time, A-APMs are not evenly distributed all through the nation, and participation amongst non-physician suppliers and sure doctor specialties remains relatively low, suggesting that further methods could also be wanted to encourage wider adoption of those fashions. Additional, MedPAC and others have famous that the scheduled conversion issue updates for qualifying A-APM clinicians might be comparatively small within the first few years after A-APM bonuses are retired, although their results will compound over time, and have cautioned that further incentives could also be wanted to stop attrition in A-APM participation throughout this transition.
Benefit-based Incentive Cost System (MIPS): Clinicians who don’t take part in A-APMs, or don’t meet the participation standards for A-APM bonus funds, are topic to further reporting necessities underneath MIPS, which adjusts funds up or down relying on a clinician’s efficiency on sure high quality metrics. As with A-APM bonuses, fee changes underneath MIPS are primarily based on efficiency two years prior. Clinicians are required to take part in MIPS if they’re eligible, however many are exempt, resembling these in sure specialties (e.g., podiatrists), these of their first yr of Medicare participation, and those that serve a low quantity of Medicare sufferers.
Cost changes underneath MIPS are required to be funds impartial. Changes are capped annually (between +9% and -9% in 2025), and financial savings generated from clinicians who incur unfavorable changes are used to fund optimistic changes for many who qualify. As a result of a relatively small share of clinicians have incurred unfavorable changes annually since MIPS was applied, optimistic changes have usually been a lot decrease than the annual cap. In 2023 as an example, roughly 600,000 clinicians obtained optimistic changes as much as +2.34%, primarily based on the 2021 performance year, whereas simply 23,000 clinicians obtained unfavorable changes right down to -9%. MedPAC estimates that another 460,000 clinicians have been ineligible for both an A-APM bonus or MIPS adjustment attributable to low Medicare affected person quantity or different exemption standards.
Clinicians who take part in MIPS have historically selected from a large set of high quality measures and different medical metrics to report on annually. Whereas this construction was supposed to offer clinicians flexibility to decide on the metrics greatest suited to their observe, it has additionally been criticized by physician groups and experts for growing the reporting burden on individuals, and for making comparisons between individuals much less clinically significant and tougher to evaluate. In an effort to handle these considerations, CMS has launched a number of extra streamlined reporting options. The latest of those permits clinicians to select from smaller, bundled subsets of reporting metrics tailor-made to specific specialties or medical situations, generally known as MIPS Value Pathways (MVPs).
MVPs have been launched in 2023 as an elective different to reporting underneath conventional MIPS, and included a preliminary set of reporting pathways geared toward particular medical contexts, resembling major care, remedy of coronary heart illness, and supportive look after neurodegenerative situations. CMS has added new MVPs annually for the reason that possibility was launched, including 6 in 2025, with the eventual goal of changing all reporting underneath conventional MIPS with MVPs in future years. The purpose of this shift is to cut back administrative burden by providing suppliers smaller, extra focused units of reporting metrics to select from, in addition to to permit for extra clinically significant assessments by evaluating outcomes amongst comparable clinicians who select to report underneath the identical MVP.
8. What considerations have been raised concerning the doctor payment schedule?
Criticism of the doctor payment schedule has centered on 4 major considerations about the way in which by which Medicare pays physicians and different clinicians. These embody: (1) the general adequacy of Medicare funds to cowl medical observe prices and incentivize participation within the Medicare program, (2) the hole in compensation between major and specialty care clinicians, (3) the affect of the AMA/RVS Update Committee (RUC) and medical specialty teams in figuring out relative fee charges for payment schedule companies, and (4) the success of the Quality Payment Program (QPP) in reaching its aim of incentivizing high quality enhancements and cost-efficient spending.
Cost Adequacy: Through the years, physician groups and some policymakers have expressed concern that fee charges underneath the doctor payment schedule have not kept pace with inflation in medical observe prices. Observe bills are one part of the relative-value calculation used to find out fee charges for payment schedule companies, however the requirement to protect funds neutrality makes it tough for CMS to extend fee for some companies with out additionally reducing fee in different areas, resembling by reducing the payment schedule conversion issue (see question 6). Statutory will increase to the conversion issue underneath MACRA should not scheduled to start till 2026, and don’t fluctuate primarily based on underlying financial situations, which can make it more difficult for some physicians to adapt to altering monetary calls for.
Core to those considerations is the chance that lack of revenues could lead on some physicians to choose out of the Medicare program, which may create access issues for Medicare beneficiaries. Nationwide surveys and different analyses have usually discovered that beneficiaries report entry to doctor companies that’s equal to, or better than, that of privately-insured people, with comparable or smaller shares reporting delays in needed care or difficulty finding a physician who takes their insurance. A recent KFF analysis discovered that simply 1% of all non-pediatric physicians had opted out of Medicare in 2024, suggesting that the present payment construction has not considerably discouraged participation. Furthermore, MedPAC estimates that virtually all Medicare claims (99.7% in 2023) are accepted on “task” and paid at the usual fee (see question 1), with beneficiaries in conventional Medicare dealing with not more than the usual 20% coinsurance fee. On the identical time, analyses by KFF and others have discovered that physicians in some specialties, resembling psychiatry, choose out of Medicare at increased charges, which can affect entry to those companies over time.
Lack of income may additionally lead some doctor practices to merge with (or be acquired by) bigger well being programs or hospitals, a course of generally known as “vertical consolidation.” Vertical consolidation could supply certain benefits to physicians, resembling higher economic system of scale for observe bills, decrease administrative burden, and entry to pricey sources resembling medical imaging gear, and could also be enticing to physicians who’re in any other case struggling to satisfy their observe prices. Whereas consolidation could also be related to some benefits to patients as properly, resembling enhancements in care integration and coordination between suppliers, it could additionally result in increased out-of-pocket prices and decrease care high quality by reducing market competition. Additional, Medicare usually pays more for a given service offered in a hospital outpatient division than it does for a similar service offered in a freestanding doctor workplace, which may result in elevated prices for beneficiaries and better program spending over time. Policymakers are presently exploring choices to align Medicare reimbursement charges between these settings, generally known as “site-neutral payment reforms.”
Main Care Compensation: A second concern with the present fee system is that Medicare doesn’t adequately pay for major care companies, as mirrored by the gap in Medicare payments between major and specialty care clinicians. Funds underneath the doctor payment schedule are usually increased for medical procedures, resembling surgical procedures and diagnostic exams, than for non-procedural companies, resembling preventive care offered throughout an workplace go to. Whereas many clinicians present a combination of procedural and non-procedural companies, major care clinicians usually dedicate a larger share of their time to non-procedural care. Additional, MedPAC has expressed concern that this imbalance encourages clinicians of all specialties to increase their use of extra pricey and worthwhile companies, resembling pointless imaging, screenings, and diagnostic exams, on the expense of high-value, however much less worthwhile, companies, resembling affected person schooling, preventive care, and coordination throughout care groups, which may affect the standard of affected person care and result in increased doctor spending over time.
MedPAC notes that medical procedures usually see gains in efficiency attributable to technological enhancements and different components, which cut back the effort and time wanted to supply them. If payment schedule charges should not adjusted to replicate these enhancements, these companies could grow to be overvalued over time. Against this, non-procedural companies usually contain extra fastened time constraints, resembling time spent speaking with sufferers or coordinating with different suppliers, and are unlikely to see comparable positive factors, contributing to the hole in compensation between these service varieties.
Resulting from funds neutrality necessities, efforts to instantly enhance fee for non-procedural companies underneath the doctor payment schedule as a way to increase funds for major care have usually necessitated across-the-board fee cuts within the type of decreases to the fee schedule conversion factor (see question 6). Additional, physicians could offset any anticipated reductions in income by increasing service volume over time, or by increasing their use of upper depth, and extra extremely compensated, service codes, leaving the hole in fee charges comparatively fixed. These constraints make it tough for CMS to meaningfully handle variations in fee between major and specialty care, and have led some policymakers to voice considerations that the present funds neutrality necessities are too inflexible.
Function of the RUC: The American Medical Affiliation (AMA) and the RUC play a considerable position in annual decision-making across the relative weighting of service codes underneath the doctor payment schedule, the first mechanism utilized by CMS to set relative fee charges for doctor and medical companies (see question 3). Whereas CMS will not be required to undertake suggestions issued by the RUC, it does so in a majority of cases. MedPAC has raised a number of methodological concerns with the information utilized by the RUC to develop its annual stories, that are largely based on recommendations from medical specialty societies. These embody an absence of transparency, in addition to low response charges and whole responses on the varied member surveys that inform medical specialty society suggestions, which make it tough for CMS to validate RUC suggestions by different means.
Different considerations raised concerning the RUC embody the overrepresentation of specialty physicians on the committee, and the potential for conflicts of curiosity when RUC members advocate modifications to relative funds for major and specialty care companies. In distinction to federal advisory committees, that are usually fashioned by Congress, the workplace of the President, or govt department businesses, the RUC is an impartial committee overseen by the AMA. Because of this, it isn’t held to the identical operating requirements as many different comparable committees, which adhere to sure standards round transparency and membership steadiness.
To make sure that payment schedule companies should not overvalued, MedPAC has recommended that CMS develop inside processes for validating RUC suggestions, resembling by accumulating information from medical practices on the variety of clinician hours devoted to commonly-billed companies. Pilot research commissioned by CMS and the Division of Well being and Human Providers (HHS) have attempted to validate the clinician time part of small subsets of payment schedule companies utilizing strategies resembling evaluation of digital well being information, direct remark of medical procedures, and independently-collected doctor surveys. These tasks could function a blueprint for future work, although implementing these and comparable strategies on a big scale would doubtless require vital time and workers funding.
Function of the QPP: QPP applications resembling the Merit-based Incentive Payment System (MIPS) and bonus funds for Superior Various Cost Mannequin (A-APM) clinicians are designed to create incentives for high quality enchancment, care coordination, and the availability of high-value companies (see question 7). Whereas the share of clinicians who qualify for A-APM bonuses has greater than tripled for the reason that QPP started (from roughly 99,000 to 386,000 within the 2017 and 2022 efficiency durations, respectively), some policymakers have argued that higher incentives are wanted to encourage suppliers to tackle the monetary dangers and excessive startup prices related to these fashions, significantly as A-APM bonus funds are phased out in favor of comparatively smaller conversion issue changes within the coming years.
Moreover, MedPAC has voiced concern that MIPS, the quality-based fee program for clinicians who don’t take part in A-APMs, imposes too massive of a reporting burden on those that take part, whereas on the identical time providing comparatively weak incentives to enhance high quality and management prices. As famous earlier, a large share of clinicians are exempt from this system, and since few individuals obtain unfavorable changes, optimistic changes are relatively modest. The executive burdens related to MIPS could also be partially addressed by the shift in direction of MIPS Value Pathways (MVPs) rather than conventional high quality reporting, and additional evaluation of this feature will doubtless take form as this system is phased in.
9. What coverage proposals have been put ahead to handle considerations with Medicare’s present doctor fee system?
Along with bipartisan legislation that instantly addresses the 2025 fee cuts that took impact January 1, 2025, policymakers and others have put ahead quite a few methods to revise the present Medicare doctor fee system. These embody measures to stabilize doctor payment schedule funds from yr to yr, present further help to major care and safety-net suppliers, and create stronger incentives for environment friendly spending, care coordination, and participation in Superior Various Cost Fashions (A-APMs).
In 2025, MedPAC recommended a one-time inflation-based enhance to doctor fee charges in 2026 (equal to the projected enhance within the Medicare Financial Index minus one proportion level), just like suggestions from past years. Whereas MedPAC has weighed the possibility of recommending annual updates for inflation, it has not carried out so up to now, focusing as a substitute on focused methods to bolster funds to major care clinicians and safety-net suppliers. For example, in mild of findings that clinicians usually obtain decrease income for treating low-income Medicare beneficiaries, MedPAC has really useful elevating fee in these instances by 15% for claims billed by major care clinicians and 5% for claims billed by non-primary care clinicians, to encourage clinicians to deal with these populations.
MedPAC has voiced help for the objectives behind the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) and the Quality Payment Program (QPP), together with the monetary incentives provided to A-APM individuals underneath present legislation (see question 7), whereas additionally recommending changes to the design of the QPP, together with the elimination of the Merit-based Incentive Payment System (MIPS). MedPAC has noted that the continued shift from conventional MIPS to MIPS Value Pathways (MVPs) addresses some considerations associated to administrative complexity and participant comparisons, however a big share of clinicians stay exempt from MIPS reporting and incentive funds have usually remained comparatively small (see question 8). Rather than MIPS, MedPAC has really useful establishing a voluntary program designed to imitate the construction of A-APMs and different alternative payment models, permitting clinicians to transition into these fashions extra regularly.
A number of payments launched within the final Congress point out curiosity in methods such elevating or modifying the funds neutrality threshold, or providing separate conversion issue updates for major and specialty care companies, which might enable CMS higher flexibility to regulate fee charges to replicate evolving coverage priorities with out necessitating a compulsory fee minimize. The Senate Finance Committee has held a number of hearings on doctor payment schedule reform, and launched a whitepaper in 2024 outlining a spread of choices to stabilize conversion factor updates from yr to yr, extend access to telehealth, and incentivize continued participation in A-APMs, amongst different reforms.
Extra just lately, Home Republicans included changes to the doctor payment schedule in a menu of potential policy actions circulated in January 2025. The Secretary of the Division of Well being and Human Providers (HHS), Robert F. Kennedy Jr., has expressed a selected curiosity in Medicare doctor fee reform, and has known as for bringing greater transparency to the operations of the AMA/RVS Update Committee (RUC) (see question 3), in addition to exploring options for lowering the position the RUC performs in annual decision-making round doctor funds.
A decade after the passage of MACRA, Congress’s final main overhaul of how Medicare pays physicians, curiosity in broader reforms to Medicare’s doctor fee system, past addressing the doctor payment cuts finalized for 2025, is gaining steam. Designing fee approaches that handle considerations raised by events to compensate physicians adequately whereas restraining spending development represents a problem for policymakers.
This work was supported partly by Arnold Ventures. KFF maintains full editorial management over all of its coverage evaluation, polling, and journalism actions.
Appendix















{kind=link}